
LOMUSTINE (CCNU) FDA-APPROVED HUMAN DRUG PRODUCT HAS BEEN REPORTED USEFUL FOR MANAGING MALIGNANT TUMORS IN DOGS
KEY POINTS:
- Lomustine (GleostineTM) has been reported to be an effective first- and second- line chemotherapy treatment for tumor-bearing dogs.1,2
- The most frequently reported toxicoses have been delayed myelosuppression, in particular neutropenia, and an elevation in serum liver enzyme laboratory values. These toxicities were reversible with supportive therapy and lomustine treatment cessation.2,3,4
- Compounded lomustine capsules should be used when accompanied with a certificate of analysis for Active Pharmaceutical Ingredient (API) content and bioavailability, because recent findings indicate that many sources’ capsules frequently contain less than 90% of the API content, and the API content often varies between capsules.5,6,7
BACKGROUND:
Lomustine (CCNU) is a nitrosourea chemotherapy agent that has been reported to be useful in the management of dogs having mast cell tumors (MCT), intracranial meningioma, epitheliotropic lymphoma (ELSA), or drug-resistant lymphoma. Lomustine has been shown to be useful as a single agent or in combination with other chemotherapy agents. Lomustine is commercially available under the trade name GleostineTM in 5 mg, 10 mg, 40 mg, and 100 mg capsules.8
Lomustine is frequently compounded; however, recent findings have demonstrated that these compounded capsules vary in API content. Additionally, studies show that there is frequently a significant difference in API content in compounded capsules from source to source and capsule to capsule.
LOMUSTINE (CCNU) HAS BEEN REPORTED TO BE EFFECTIVE IN THE MANAGEMENT OF CANINE ELSA.1
Study 1. In this retrospective study, 46 dogs with ELSA were treated with lomustine.1 The median number of treatment cycles was four (range, 1–11 cycles) with a median starting dose of 60 mg/m2 (range, 30–95 mg/m2).
- 14 dogs received lomustine as first line therapy.
- 32 dogs had been dosed with some other form of therapy prior to lomustine usage.
- Overall response rate (complete response and partial response [CR + PR]) was 83%. [Figure 1]
- 29 of the 46 dogs had treatment discontinued because of progressive disease.
- 8 of the 46 dogs had treatment discontinued because of dose-related toxicity (thrombocytopenia or increased liver enzyme activity).
LOMUSTINE-INDUCED HEPATOPATHY MAY OCCUR IN AS LITTLE AS TWO TREATMENT CYCLES BUT IS EFFECTIVE IN STABILIZING ADVANCED MCT IN DOGS.2
Study 2. In this prospective study, 81 dogs with advanced stage MCT were randomized to four cycles of 70 mg/m2 lomustine treatment every three weeks.2
- 16 dogs completed the assigned four-cycle treatment protocol.
- 65 dogs had treatment discontinued.
- 26 dogs developed progressive disease during the protocol.
- 27 dogs developed hepatopathy after two cycles of lomustine.
- Overall response rate (CR + PR) for the 16 dogs completing the protocol was 6% (1 of the 16 dogs).
- 7 of the 16 dogs had a stable response with the assigned protocol.
LOMUSTINE TREAMENT IN DOGS RESULTS IN DELAYED BUT REVERSIBLE TOXICITY.3,4
STUDY 3. IN THIS RETROSPECTIVE STUDY, 206 DOGS WERE TREATED WITH LOMUSTINE AS PART OF A SINGLE-AGENT OR MULTI-AGENT PROTOCOL.3
- 10 dogs had treatment discontinued because of dose-related toxicity (thrombocytopenia, gastrointestinal toxicity, hepatoxicity, anemia, and/or renal failure). 30 dogs had treatment reduced because of dose-related toxicity.
Study 4. In this study, 179 dogs were treated with lomustine given as a single dose of 50– 110 mg/m2 with a variable dose interval (minimal three-week interval between doses).4
- 11 dogs developed hepatic toxicity after receiving treatment.
- Overall response rate (CR + PR) for the 11 dogs at diagnosis of hepatoxicity was 90.9% (10 of the 11 dogs).
- Median duration to detection of hepatic toxicity from last dose of lomustine was 11 weeks (range, 2–49 weeks).
- Median number of lomustine doses and median total cumulative lomustine dosages were significantly higher in dogs with lomustine-induced hepatotoxicity (4 doses; 350 mg/m2) than dogs showing no signs of hepatotoxicity (3 doses; 230 mg/m2).
COMPOUNDED LOMUSTINE VARIES AND MAY NOT REFLECT THE PRESCRIBED AMOUNT.5,6
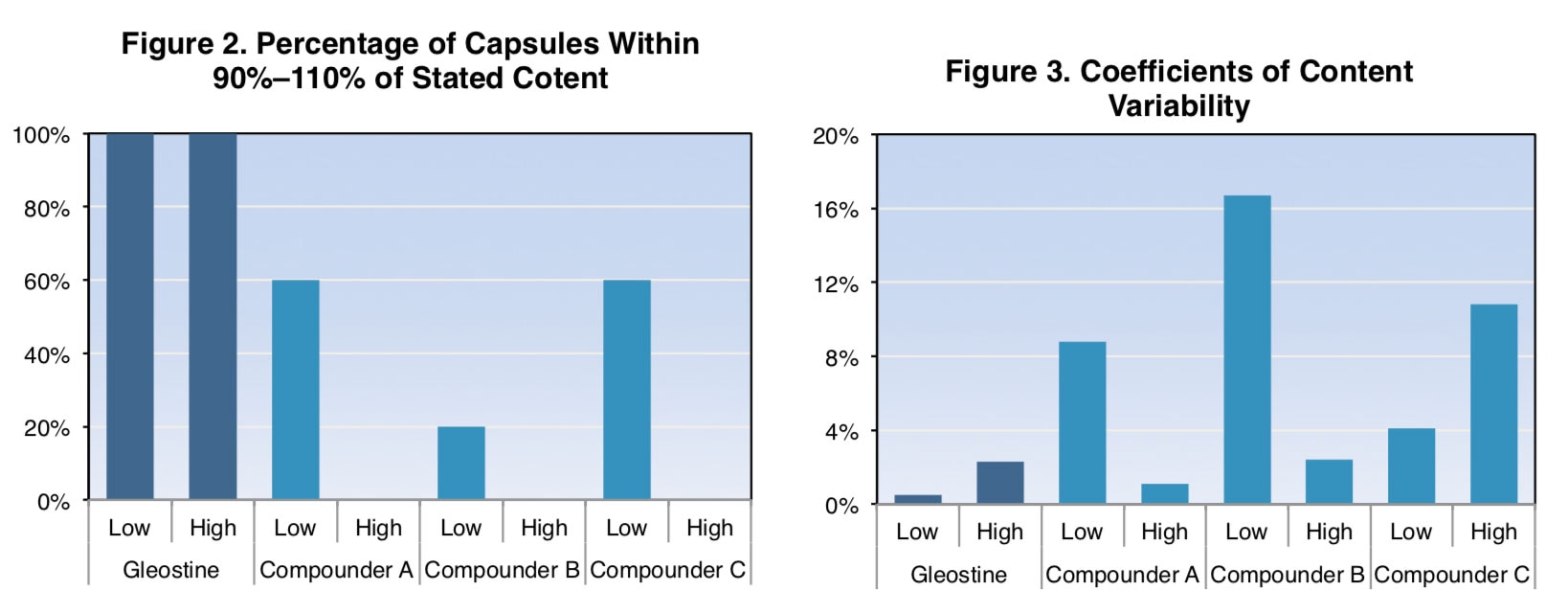
Study 5. In this laboratory analysis, the lomustine drug content of five low-dose (10 mg capsules) and five high-dose (40 mg capsules) lomustine capsules from three compounders and one FDA-approved manufacturer was assessed by validated high-pressure liquid chromatography (HPLC) with ultraviolet (UV) detection method.5
- GleostineTM capsules were all within the a priori acceptable limit of 90%–110% of the stated content (range, 104%–110%). [Figure 2]
- Compounded capsules were often outside the a priori acceptable limit of 90%–110% of the stated content (range, 78%–95%).
- Compounded capsules had a failure rate of 40%–100%.
- Coefficients of variation for the compounded capsules were frequently high, while the variability for GleostineTM capsules was relatively low. [Figure 3]
- Coefficients of variation for the compounded capsules were 4.1%–16.7% for low- dose formulas and 1.1%–10.8% for high-dose formulas.
- Coefficients of variation for GleostineTM capsules were 0.5% for the low-dose and 2.3% for the high-dose formula.
STUDY 6. This two-part study involved (1) a retrospective study assessing the severity and frequency of neutropenia in tumor-bearing dogs treated with GleostineTM or compounded lomustine, and (2) a laboratory analysis of the potency of compounded lomustine.
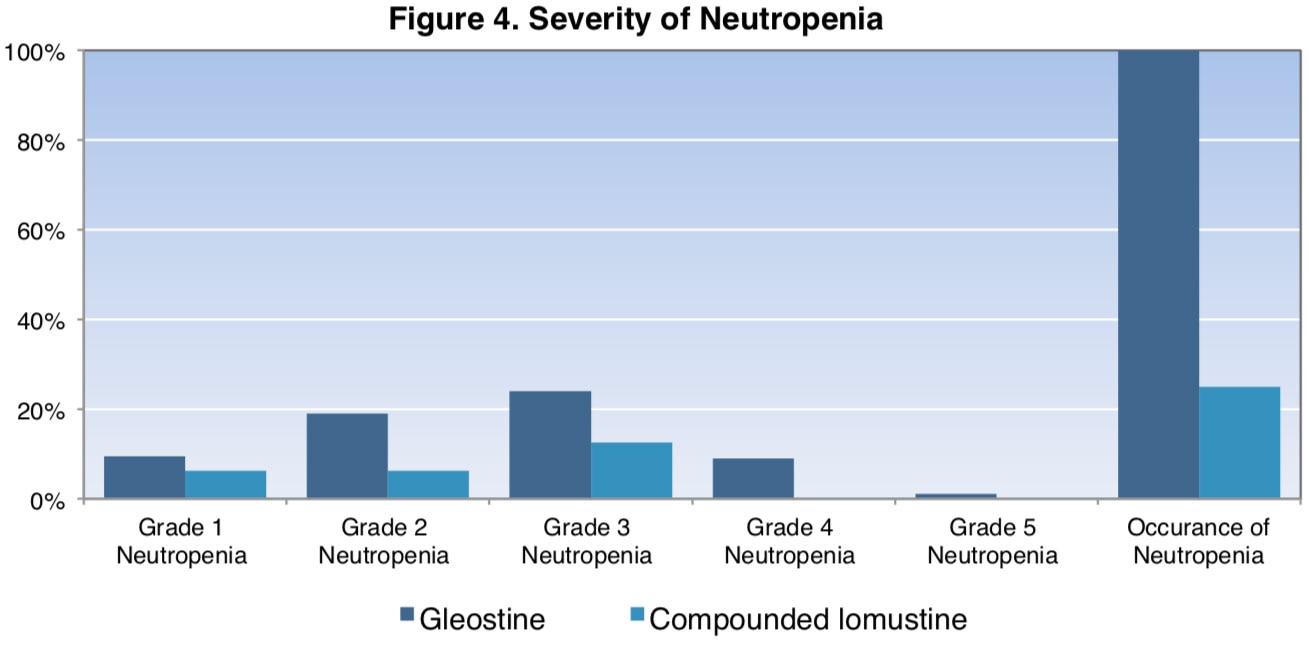
In the retrospective study, 21 dogs were treated with GleostineTM and 16 dogs received compounded lomustine obtained from a single compounding pharmacy. Severity (grade) of neutropenia was determined using the Veterinary Cooperative Oncology Group – Common Terminology for Adverse Effects, and nadir neutrophil counts were performed 6 to 10 days after lomustine administration.
- Frequency and severity of neutropenia associated with lomustine administration were significantly lower in dogs treated with compounded lomustine compared to GleostineTM.
- All 21 dogs (100%) treated with GleostineTM were neutropenic after treatment. The median neutrophil count one week after treatment was 638/μL (range, 42–2,941/μL).
- 15 of the 21 dogs (71%) developed grade 3 or higher neutropenia. [Figure 4]
- 4 of the 16 dogs (25%) treated with compounded lomustine became neutropenic. The median neutrophil count one week after treatment was 3,520/μL (range, 560–20,697/μL).
- 2 of the 16 dogs (12.5%) developed grade 3 neutropenia.
- 3 of the 16 dogs (19%) either had no change (1 dog) or an increase (2 dogs) in neutrophil count from baseline to nadir.
In the laboratory analysis, the lomustine drug content of 5 mg lomustine capsules from five compounders was tested using HPLC with UV detection.
- Compounded capsules varied significantly in potency (range, 50%–115% of stated content).
- Only capsules from one of the five compounders were within 90%–110% of the stated content.
CONCLUSION
The high response rate and low occurrence of fatal toxicity reported in these studies support lomustine as a treatment option for dogs. However, findings from two laboratory analyses indicate that compounded lomustine capsules have wide variability of API, and a majority of the tested compounded capsules were reported to contain less than 90% of the stated active drug content. Laboratory analysis further indicates that GleostineTM capsules contain relatively uniform amounts of lomustine. In addition, researchers observed significantly higher frequency and severity of neutropenia in dogs treated with GleostineTM compared to dogs treated with compounded lomustine.
TREATMENT RECOMMENDATIONS
The data from these studies illustrate the potential benefits of using GleostineTM alone or as part of a combination regimen for the treatment of dogs with MCT, intracranial meningioma, ELSA, or drug-resistant lymphoma. However, incorrect dosages could result in treatment failure, unpredictable results, and potentially enhanced neoplasia chemotherapy resistance. Therefore, compounded lomustine—which has been shown to carry risks of inaccurately dosing a patient due to potential content failure and variability—should be used cautiously. If compounding is done, GleostineTM should be utilized to ensure minimal variability in content and higher potency; unregulated, unapproved API sources should not be used.
1 Ribson, R. E., et al. (2006). Response of canine cutaneous epitheliotropic lymphoma to lomustine (CCNU): A retrospective study of 46 cases (1999–2004). J Vet Intern Med., 20, 1389–1397.
2 Vail, D. M., et al. (2012). A randomized trial investigating the efficacy and safety of water soluble micellar paclitaxel
(Paccal Vet) for treatment of nonresectable grade 2 or 3 mast cell tumors in dogs.” J Vet Intern Med., 26, 598–607.
3 Heading, K. L., L. K. Brockley, & P. F. Bennet. (2011). CNNU (lomustine) toxicity in dogs: A retrospective study (2002–07). Australian Veterinary Journal, 89 (4), 109–116.
4 Kristal, O., et al. (2004). Hepatoxicity associated with CCNU (lomustine) chemotherapy in dogs. J Vet Intern Med., 18, 75–80.
5 KuKanich, B., M. Warner, & K. Hahn (2017). Analysis of lomustine drug content in FDA-approved drug product and
compounded lomustine capsules. J Amer Vet Med Assoc., 250, 322-326.
6 Burton, J. H., et al. (2016). Frequency and severity of neutropenia associated with Food and Drug Administration approved and compounded formulations of lomustine in dogs with cancer. J Vet Intern Med., 30, 242–246.
7 Burton J., et al. (2014). Decreased frequency and severity of neutropenia associated with
compounded formulations of CCNU. Presented at the Veterinary Cancer Society Annual Conference, St. Louis, MO.
8 NextSource Biotechnology. (2013). Lomustine (CCNU) [package insert]. Retrieved from